

O-PED-16 - Endoscopic third ventriculostomy in a patient with extremely narrow interpeduncular and prepontine cisterns
1Department of Neurosurgery and Spine Unit, Hospital Universitario Marqués de Valdecilla and Fundación Instituto de Investigación Marqués de Valdecilla (IDIVAL), Santander. 2Department of Neurosurgery, Hospitales Universitarios Virgen del Rocío, Seville. 3Department of Neurosurgery, Complejo Hospitalario de Toledo.
Objectives: Prepontine cistern status and unidentifiable third ventricular floor anatomy are recognized factors affecting outcome of an endoscopic third ventriculostomy. Here we present a video of an endoscopic third ventriculostomy in a patient with hydrocephalus and narrow interpeduncular and prepontine cisterns. We describe the technical pitfalls and review useful anatomical landmarks.
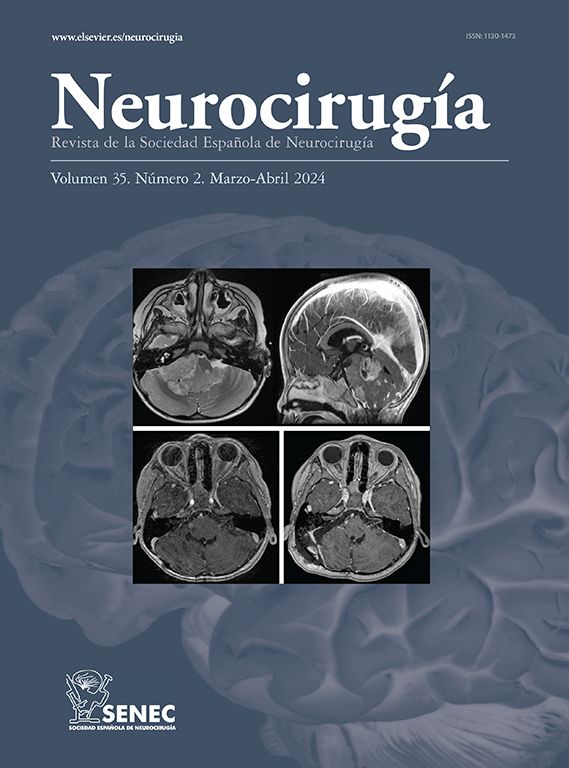
Material and methods: A 13-year-old female patient, with a one-year history of headache and progressive ataxia. MRI showed an obstructive hydrocephalus secondary to a lesion compatible with a mesencephalic tectum glioma. The third ventricle floor was bowing to the sellar region. The prepontine cistern was virtually collapsed and the posterior clinoid processes protruded towards the third ventricle. An endoscopic third ventriculostomy was performed using a 6 mm rigid endoscope with a 0º lens (Minosp, Aesculap, USA). Third floor ventricle anatomical landmarks were identified. The posterior clinoid process and the dorsum sellae helped to slide the bipolar tip and the fogarty catheter directly to the tuber cinereum, in the narrow space between the dorsum sellae and the mammillary bodies. Then, Lilliequist membrane was opened using the same technique.
Results: There were not any surgical complications. Patient´s ataxia and headache episodes improved progressively after the procedure. Postoperative MRI confirmed the ventriculostomy permeability despite any changes in the prepontine cistern.
Conclusions: Although prepontine cistern status could be an important factor for the endoscopic ventriculostomy outcome, it is not an absolute contraindication. Recognition of prepontine cistern collapse in the preoperative planning, intraoperative anatomical landmarks and appropriate technique are important factors for a good outcome.



