






The semisitting position offers surgical advantages for posterior fossa and pineal region procedures but remains controversial due to potential complications such as venous air embolism (VAE) and tension pneumocephalus. This study reviews a 20-year single-center experience to assess its safety, complication profile, and clinical outcomes under a standardized monitoring protocol.
Materials and methodsThis retrospective cohort study included all consecutive patients undergoing neurosurgical procedures in the semisitting position at our tertiary center from January 2004 to December 2024. Patients were monitored using a standardized protocol including precordial Doppler ultrasonography, end-tidal CO2 monitoring, and central venous catheter placement. Patient demographics, surgical details, perioperative complications, and clinical outcomes were systematically analyzed. Venous air embolism (VAE) and other significant adverse events were specifically documented. Statistical analyses included univariate and multivariate logistic regression analyses to identify potential risk factors for complications.
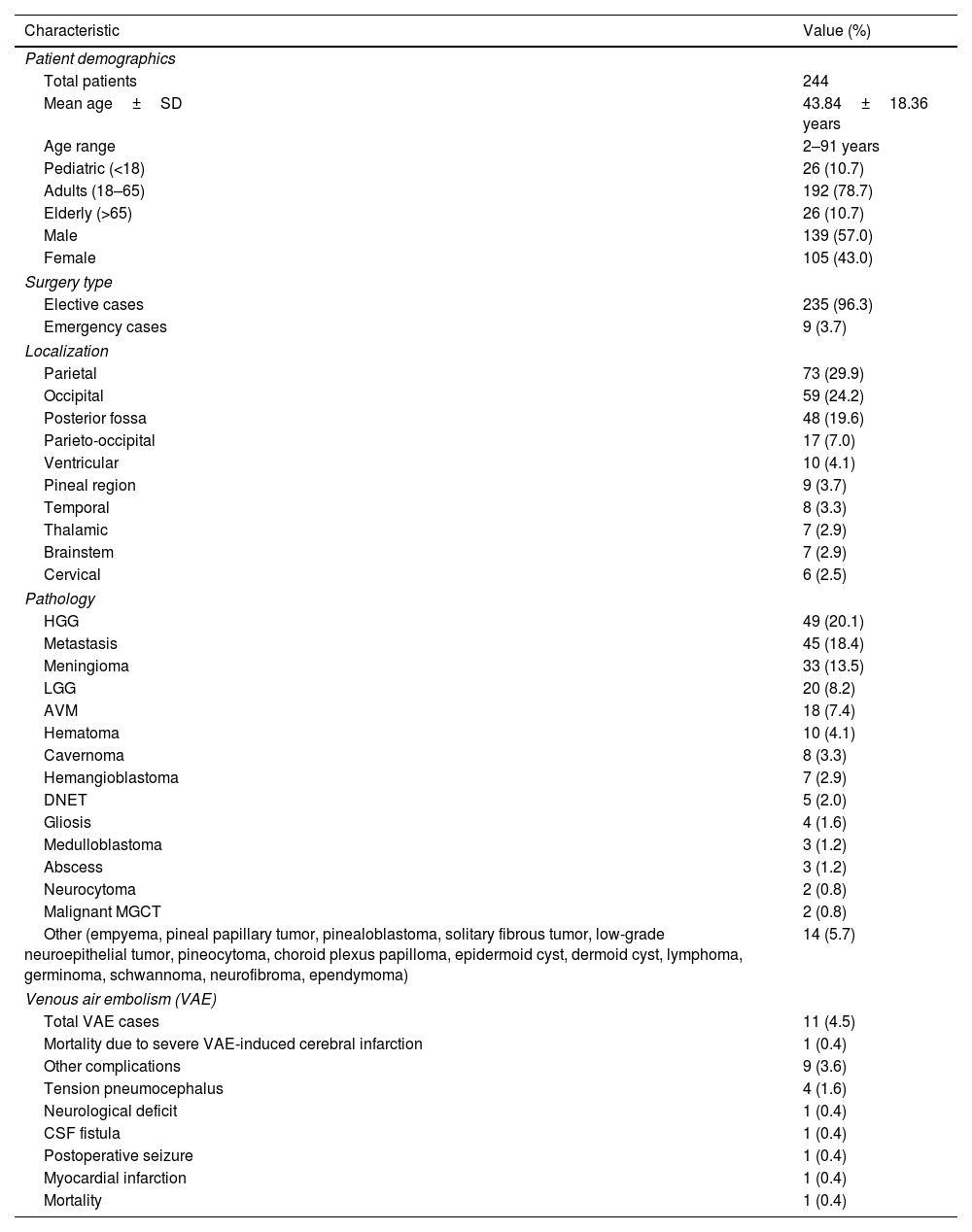
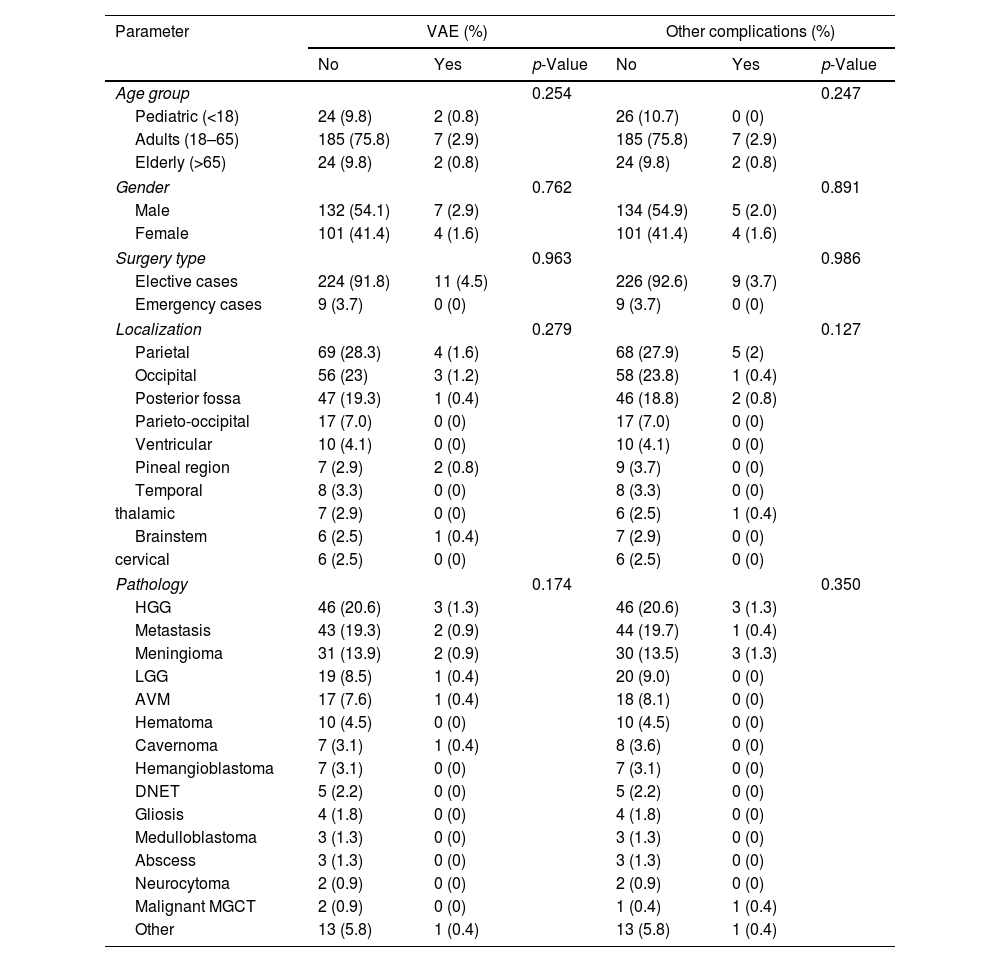
ResultsA total of 244 patients underwent surgery in the semisitting position, with a mean age of 43.8±18.4 years. The most common surgical localizations were the parietal and occipital regions, followed by the posterior fossa. The incidence of VAE was 4.5% (n=11), including one fatal cerebral infarction. Other complications occurred in 3.6% of cases, including tension pneumocephalus (1.6%), neurological deficit, cerebrospinal fluid leakage, postoperative seizure, myocardial infarction, and ischemic infarction (each 0.4%). Multivariate analysis did not identify significant predictors of complications.
ConclusionsThe semisitting position remains a safe and effective neurosurgical approach when executed with rigorous protocols and vigilant monitoring. With careful management, these risks can be effectively mitigated, underscoring their continued utility in suitable cases, particularly for surgeries involving the posterior fossa and pineal region.
La posición semisentada ofrece ventajas quirúrgicas para los procedimientos en la fosa posterior y la región pineal, pero sigue siendo controvertida debido a posibles complicaciones como la embolia aérea venosa (EAV) y el neumoencéfalo a tensión. Este estudio revisa una experiencia de 20 años en un único centro para evaluar su seguridad, perfil de complicaciones y resultados clínicos bajo un protocolo de monitorización estandarizado.
Material y métodosEste estudio de cohorte retrospectivo incluyó a todos los pacientes consecutivos sometidos a procedimientos neuroquirúrgicos en posición semisentada en nuestro centro terciario entre enero de 2004 y diciembre de 2024. Los pacientes fueron monitorizados mediante un protocolo estandarizado que incluía ecografía Doppler precordial, monitorización de CO2 al final de la espiración y colocación de un catéter venoso central. Se analizaron sistemáticamente los datos demográficos, detalles quirúrgicos, complicaciones perioperatorias y resultados clínicos. La embolia aérea venosa (EAV) y otros eventos adversos significativos fueron documentados específicamente. El análisis estadístico incluyó análisis univariado y multivariado de regresión logística para identificar posibles factores de riesgo de complicaciones.
ResultadosUn total de 244 pacientes fueron intervenidos en posición semisentada, con una edad media de 43,8 ± 18,4 años. Las localizaciones quirúrgicas más frecuentes fueron las regiones parietal y occipital, seguidas por la fosa posterior. La incidencia de EAV fue del 4,5% (n=11), incluyendo un caso fatal de infarto cerebral. Otras complicaciones se presentaron en el 3,6% de los casos, incluyendo neumoencéfalo a tensión (1,6%), déficit neurológico, fuga de líquido cefalorraquídeo, crisis epilépticas postoperatorias, infarto de miocardio e infarto isquémico (cada uno con una incidencia del 0,4%). El análisis multivariado no identificó predictores significativos de complicaciones.
ConclusiónLa posición semisentada sigue siendo una estrategia neuroquirúrgica segura y eficaz cuando se aplica con protocolos rigurosos y monitorización estrecha. Con una gestión cuidadosa, estos riesgos pueden mitigarse eficazmente, lo que respalda su utilidad continuada en casos seleccionados, especialmente en cirugías de la fosa posterior y la región pineal.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



