


Las fístulas de líquido cefalorraquídeo hacia las cavidades nasosinusales (rinolicuorreas) constituyen un proceso con dificultades diagnósticas y también terapéuticas. El abordaje transnasal endoscópico es el método de elección, pero con numerosas variantes posibles. El objeto de este trabajo es hacer una revisión crítica del protocolo diagnóstico y terapéutico que nosotros aplicamos desde hace 11años.
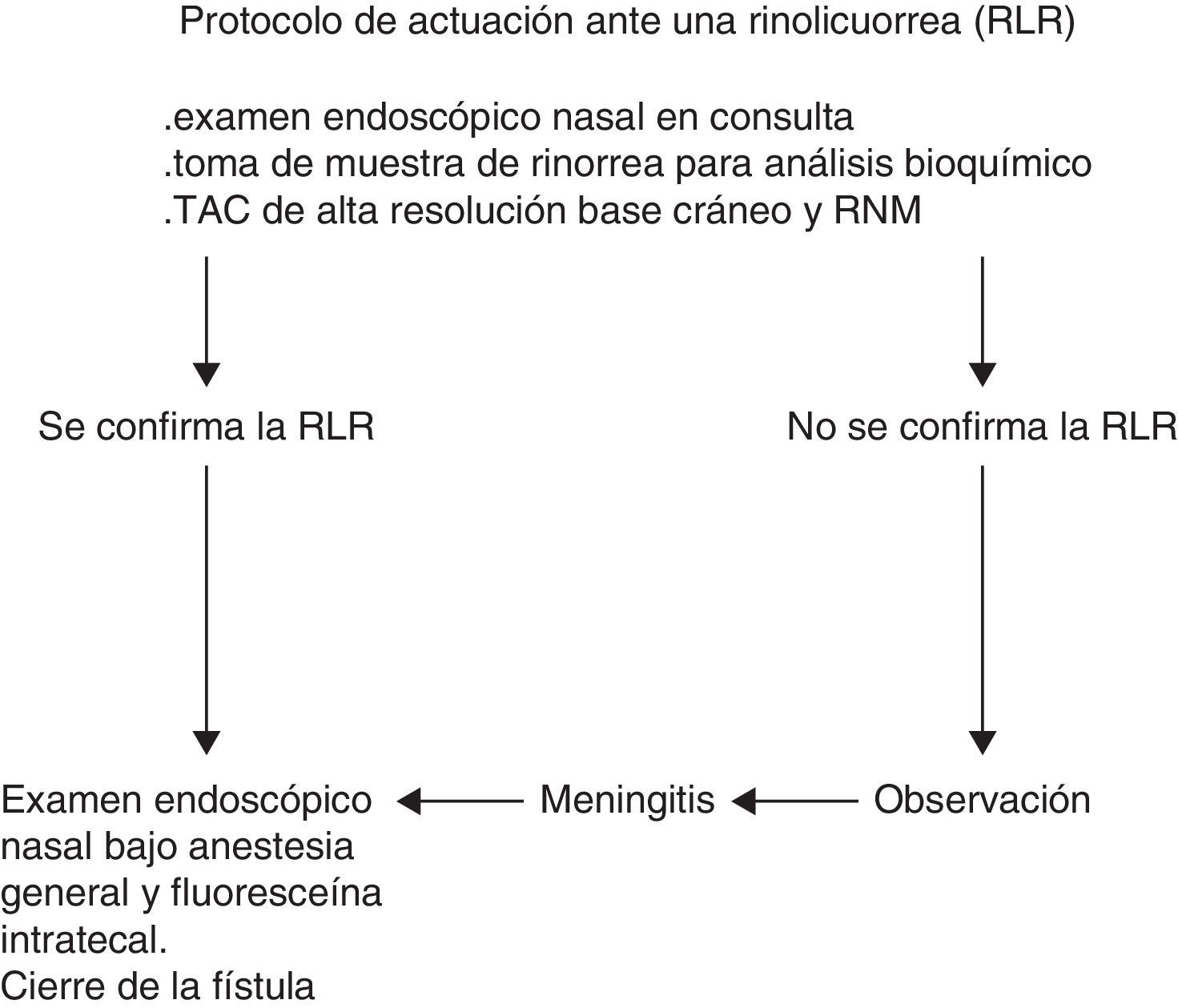
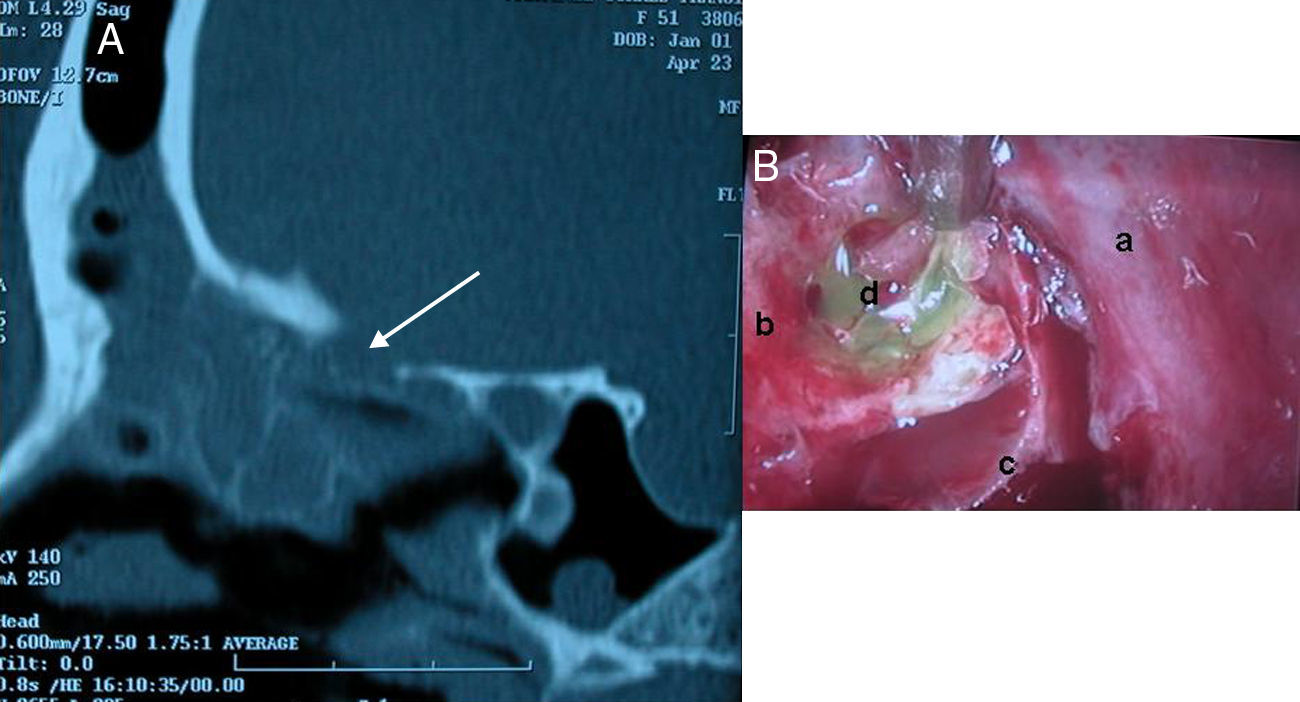
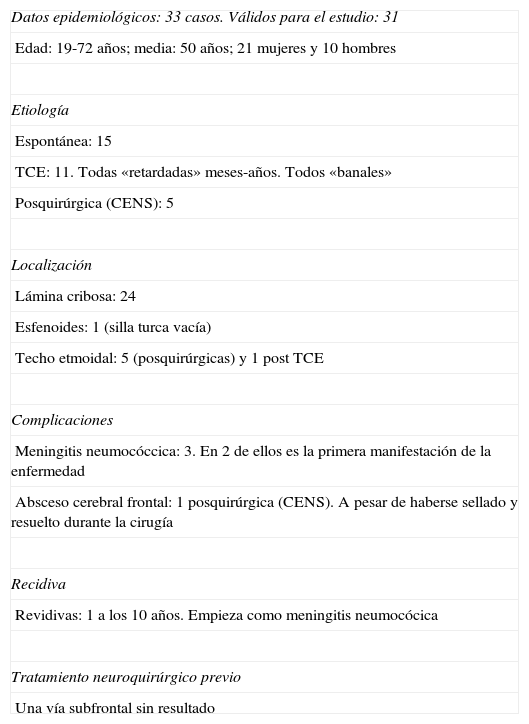
Material y métodosTreinta y un pacientes intervenidos. El diagnóstico se fundamenta en el análisis bioquímico de la rinorrea, la TAC y la RNM. Tratamiento: se realiza mediante cirugía endoscópica tras la inyección intratecal preoperatoria de 2cc de fluoresceína al 5%. El cierre se efectúa mediante un injerto libre de mucosa de cornete medio superpuesta, «overlay».
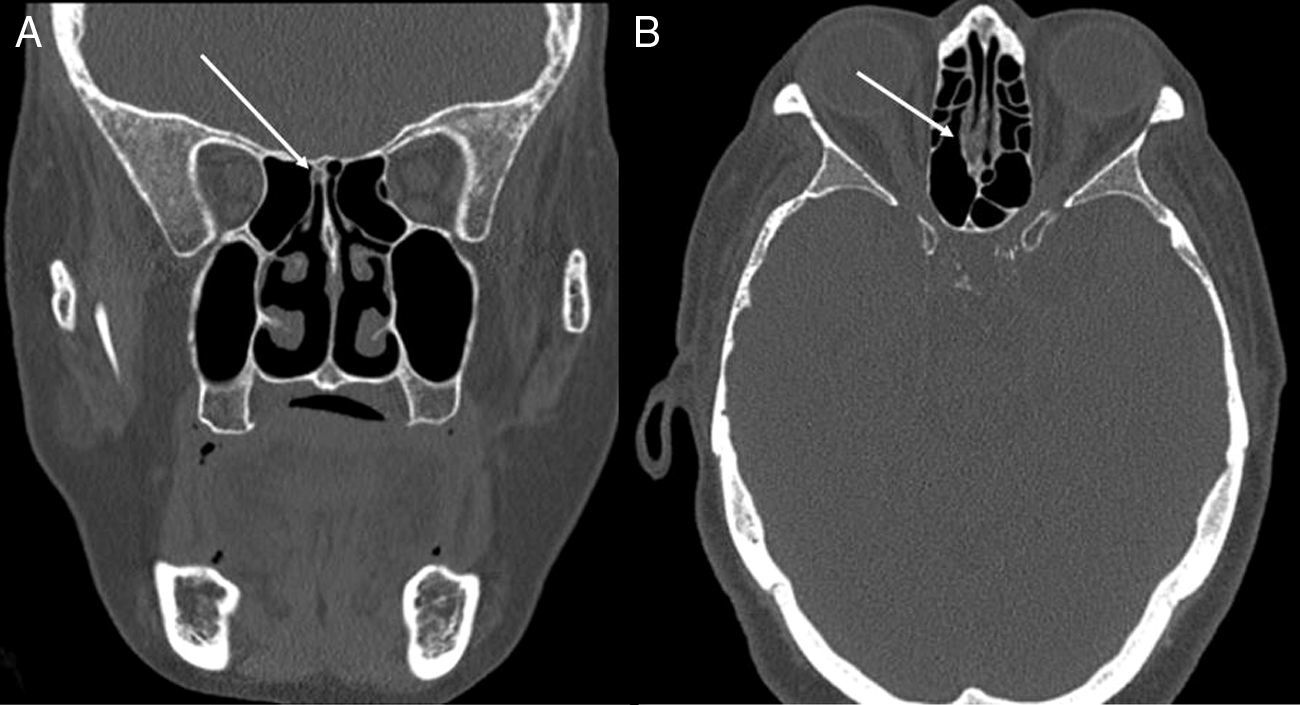
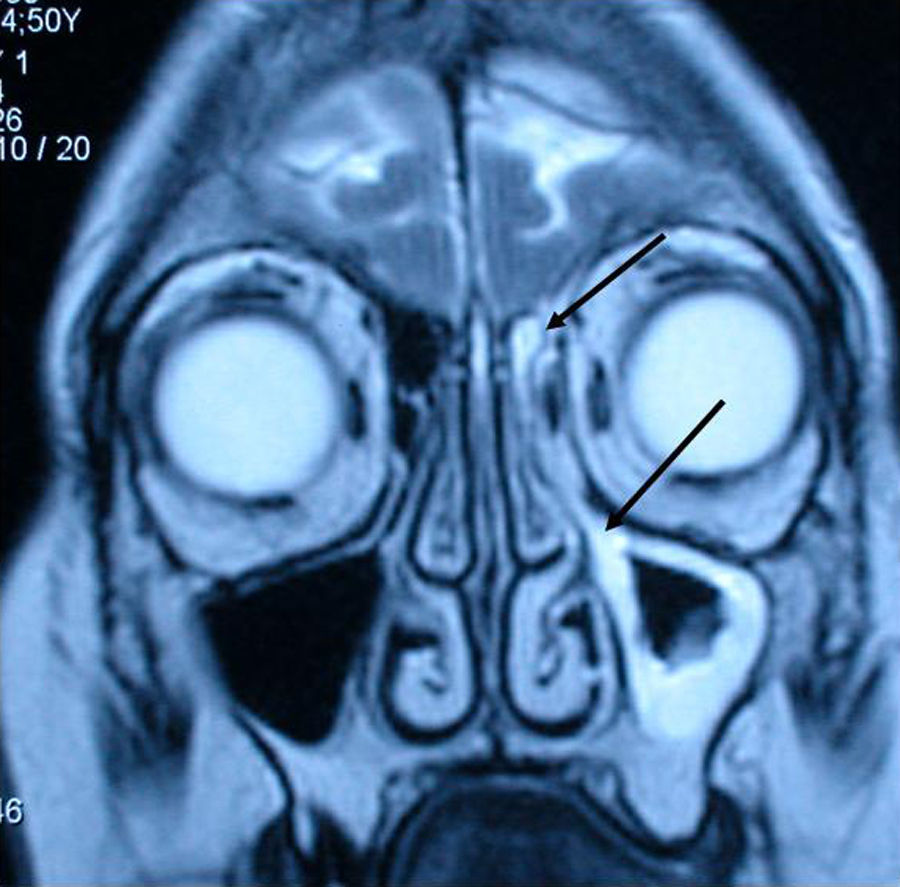
ResultadosDos pacientes presentaron meningitis como primer signo. En todos los pacientes se diagnosticó la rinolicuorrea mediante el análisis bioquímico del moco. La TAC y la RNM dieron indicios claros para la localización del punto de fuga. El defecto basicraneal fue siempre menor de 1cm. La fluoresceína permitió visualizar la zona fistulosa sin necesidad de otros instrumentos y no tuvo efectos secundarios. Un paciente sufrió un absceso frontal en el postoperatorio que evolucionó favorablemente. Todas las fístulas se cerraron y solo hubo una recidiva a los 10años que empezó como una meningitis neumocócica.
Discusión y conclusionesNuestro protocolo quirúrgico, fundamentado en el uso de fluoresceína intratecal y la colocación de un injerto libre de mucosa nasal sobrepuesto —«overlay»— sobre la zona fistulosa consigue resultados muy satisfactorios a largo plazo para el tratamiento de las rinolicuorreas por pequeños defectos basicraneales.
Cerebrospinal fluid leaks to the sinonasal cavities (rhinoliquorrhoea) represent a process with diagnostic and therapeutic difficulties. The endoscopic transnasal approach is the method of choice, but with many possible variants. The purpose of this paper was to make a critical review of our diagnostic and therapeutic protocol used for 11years.
Material and methodsWe operated on 31patients. The diagnosis was based on the biochemical analysis of rhinorrhoea, CT and MRI. Treatment: endoscopic nasal surgery after preoperative intrathecal injection of 5% fluorescein (2cc). Closure was performed using a free overlay graft from middle turbinate mucosa.
ResultsTwo patients had meningitis as the first sign. All patients were diagnosed by biochemical analysis of rhinorrhoea. CT and MRI gave clear evidence of the leakage location. The skull base defect was always less than 1cm. Fluorescein allowed clear visualisation of the fistulous area without other instruments and produced no side effects. One patient had a postoperative frontal abscess, which evolved favourably. All fistulas were closed and there was only one recurrence at 10years, which debuted as pneumococcal meningitis.
Discussion and conclusionsOur surgical protocol, based on the use of intrathecal fluorescein and free grafting of middle turbinate mucosa overlay onto the fistulous area, achieves successful long-term results in the management of rhinoliquorrhoea secondary to small skull base defects.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



