


Exponer la experiencia con el abordaje pterional transcigomático en el tratamiento de la patología neuroquirúrgica de la base de cráneo situada en la fosa craneal media y zonas vecinas.
Material y métodoEstudio retrospectivo de la patología, resultados quirúrgicos y complicaciones obtenidos en 31 casos intervenidos entre 2009 y 2011 usando un abordaje pterional transcigomático.
ResultadosSe han intervenido lesiones del ala del esfenoides (25,9%), afectando varias regiones por su crecimiento invasivo (19,5%), del lóbulo temporal (16,1%) y del seno cavernoso (12,9%), involucrando el resto al suelo de la fosa media, cavum de Meckel, región incisural, cisternas y región infratemporal. La naturaleza de las lesiones intervenidas fue la siguiente: meningioma benigno (42%), tumor parenquimatoso (19,5%), patología vascular (12,9%), lesiones inflamatorias (6,4%), meningioma atípico (6,4%), tumor epidermoide (6,4%), neurinoma (3,2%) y carcinoma pobremente diferenciado infratemporal (3,2%). La mayor parte de las veces el abordaje fue combinado extra-intradural (58,1%), y con menor frecuencia extradural (16,1%) o intradural (25,8%) puro. Las complicaciones relacionadas con el abordaje fueron menores: hematomas en la herida que no requirieron tratamiento (67,8%), paresia facial superior transitoria (9,7%), de disfunción transitoria de articulación temporomandibular (12,9%) y atrofia del músculo temporal (16,2%). No hubo ningún caso de aflojamiento de material ni problemas estéticos relacionados con la osteotomía y osteosíntesis del arco cigomático.
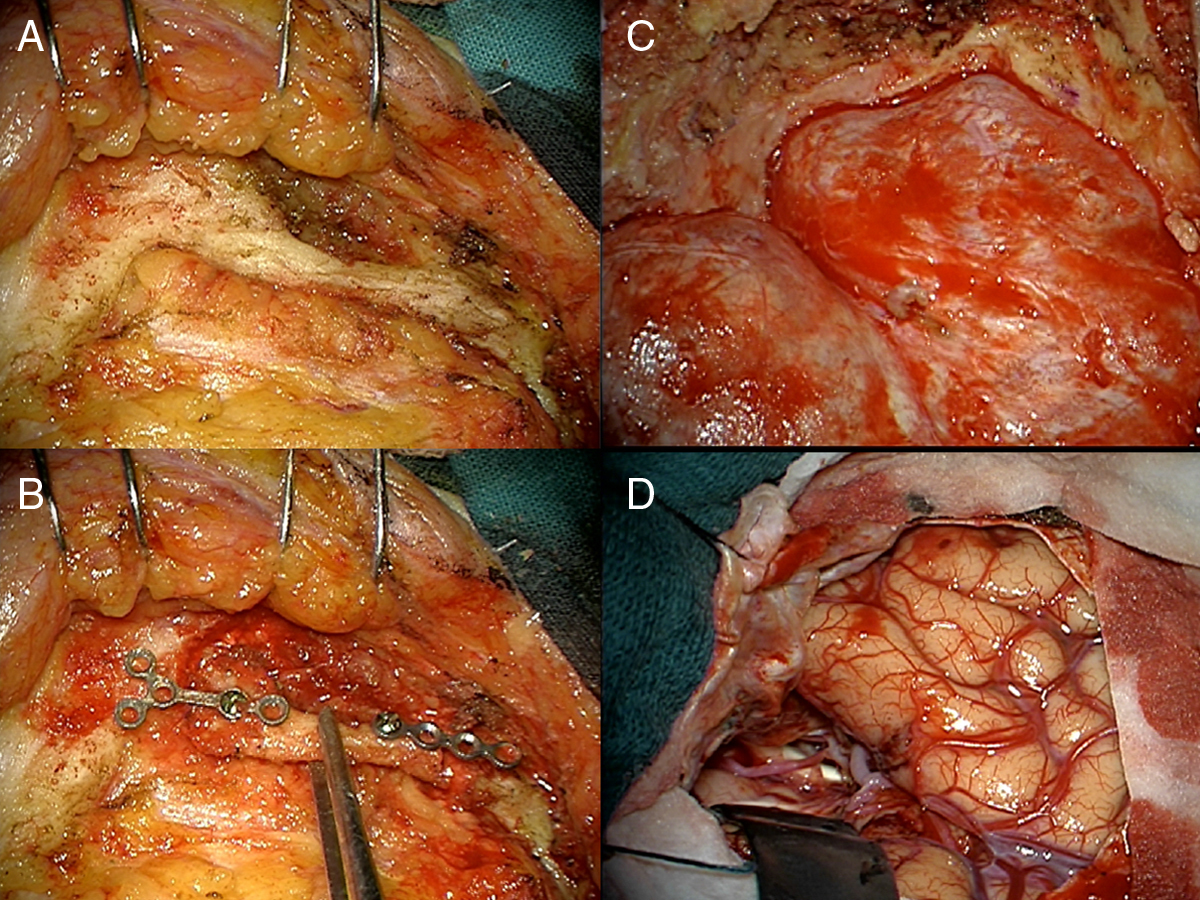
ConclusionesLa modificación del abordaje pterional asociando una osteotomía del arco cigomático, que permite rebatir el músculo temporal de toda la fosa temporal y exponer así toda su superficie para completar la craneotomía temporal hasta la base de la fosa media, nos facilita el acceso para tratar patología de la misma o utilizarla como corredor para el acceso a zonas vecinas.
To present our experience with the transzygomatic pterional approach in the treatment of neurosurgical pathology of the base of the skull located in the middle cranial fossa and surrounding areas.
MethodA retrospective study of pathological findings, surgical outcomes and complications in a series of 31 cases operated on between 2009 and 2011 using a transzygomatic pterional approach.
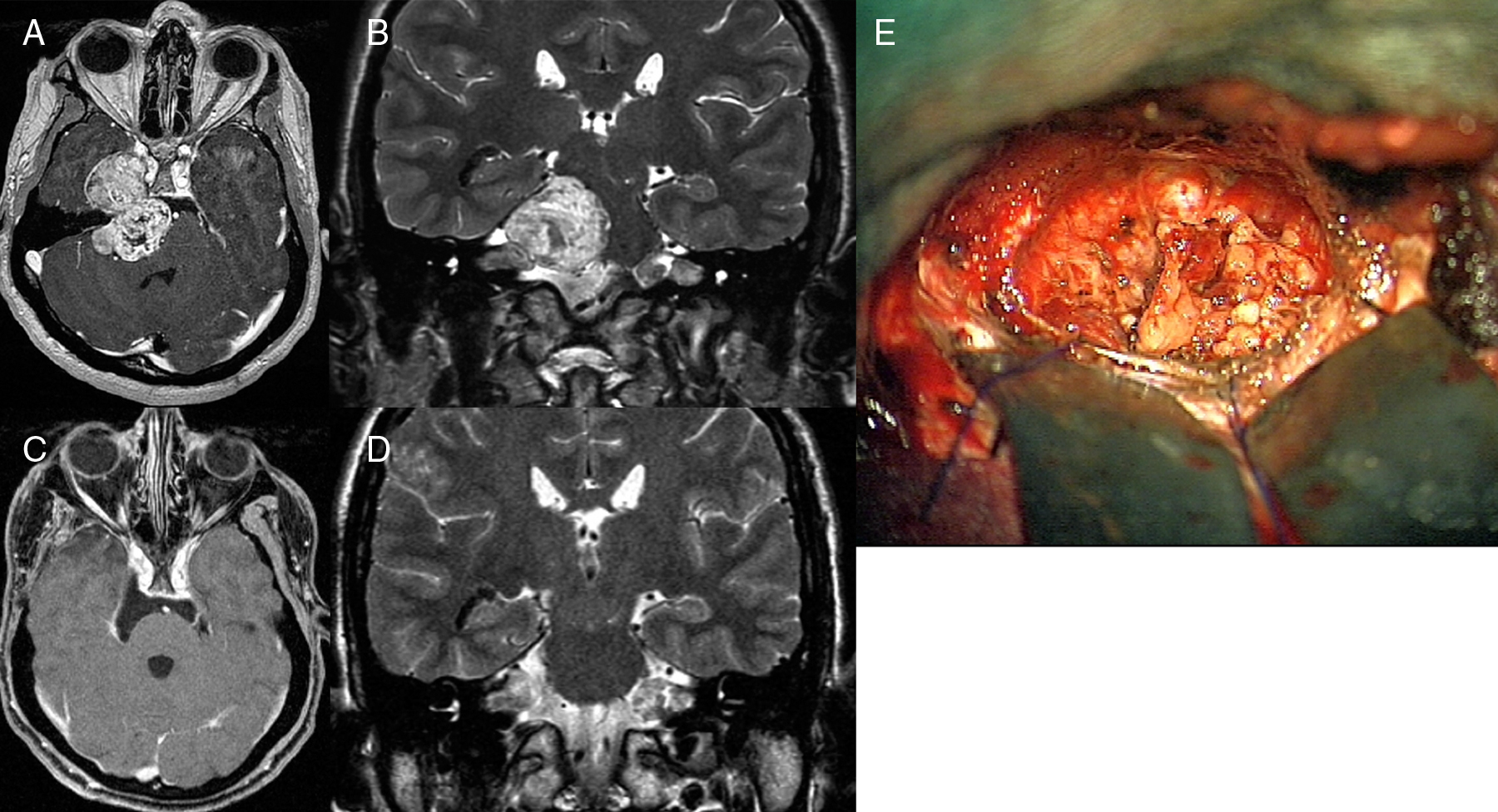
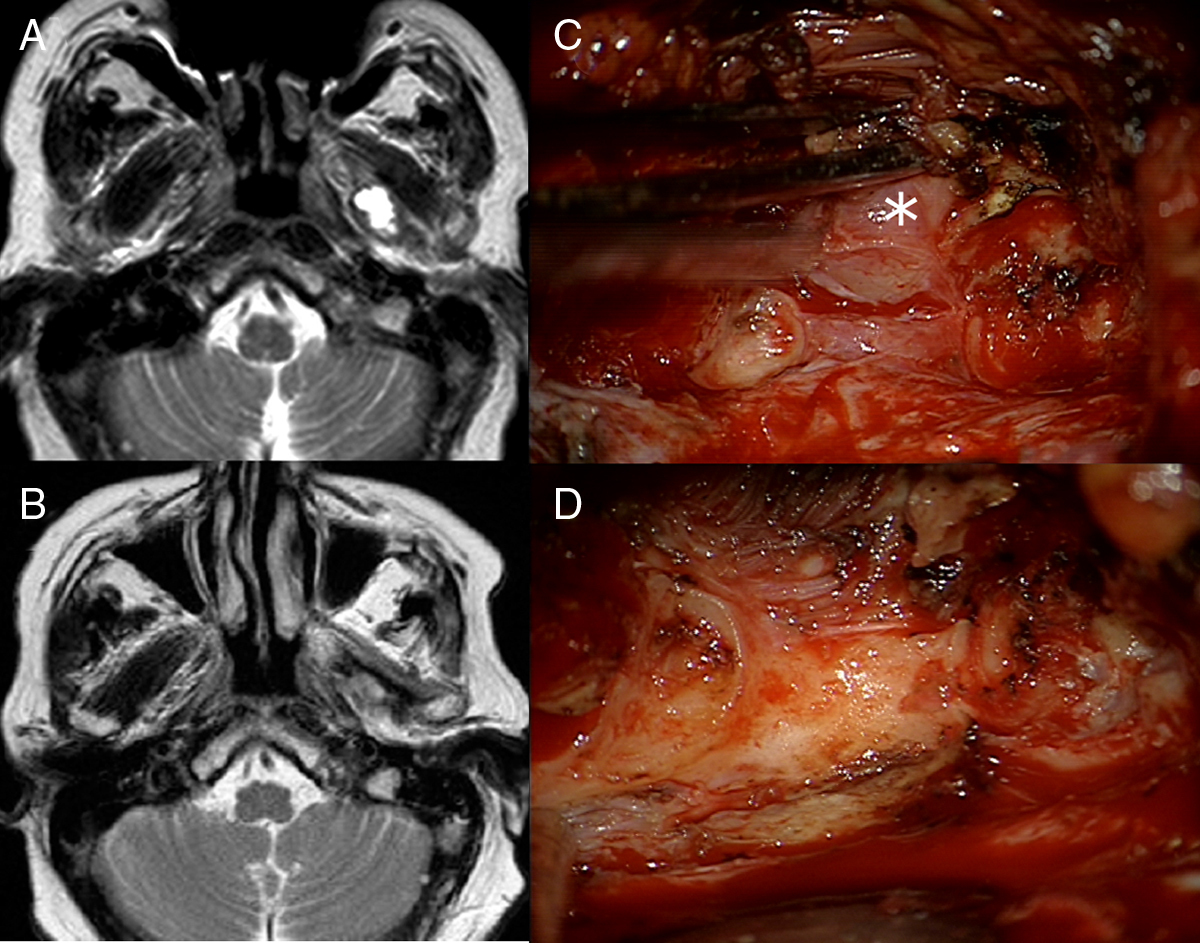
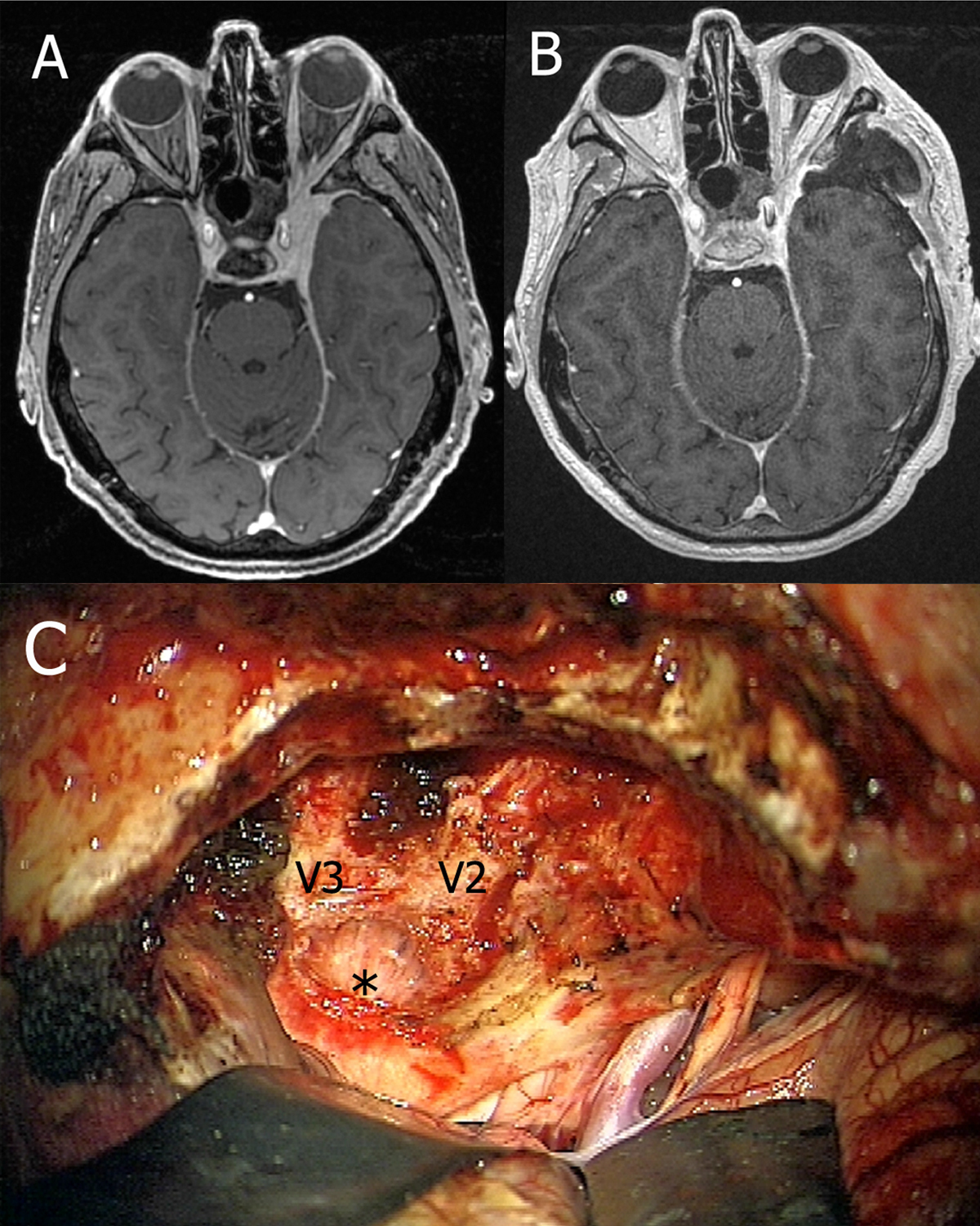
ResultsThe lesions involved the sphenoid wing (25.9%), several regions due to invasive growth pattern (19.5%), the temporal lobe (16.1%) and cavernous sinus (12.9%). The others were located in the floor of the middle fossa, Meckel's cave, incisural space, cisterns and infratemporal region. The pathological nature of the lesions was: benign meningioma (42%), temporal lobe tumour (19.5%), vascular disease (12.9%), inflammatory lesions (6.4%), atypical meningioma (6.4%), epidermoid cyst (6.4%), neurinoma (3.2%) and poorly differentiated infratemporal carcinoma (3.2%). The approach was usually combined extra-intradural (58.1%) and, less frequently, just extradural (16.1%) or intradural (25.8%). Approach-related complications were minor: haematomas in the wound not requiring treatment (67.8%), superior transient facial paresis (9.7%), transient temporomandibular joint dysfunction (12.9%) and atrophy of the temporal muscle (16.2%). There were no hardware-related complications or cosmetic issues related to the osteotomy and posterior osteosynthesis of the zygomatic arch.
ConclusionsThe pterional approach combined with osteotomy of the zygomatic arch allows mobilising the temporalis muscle away from the temporal fossa, consequently exposing its entire surface to complete the temporal craniotomy up to the middle fossa; it helps to access and treat pathology in this region or it can be used as a corridor to approach surrounding areas.
Article
![]()
If it is the first time you have accessed you can obtain your credentials by contacting Elsevier Spain in suscripciones@elsevier.com or by calling our Customer Service at902 88 87 40 if you are calling from Spain or at +34 932 418 800 (from 9 to 18h., GMT + 1) if you are calling outside of Spain.
If you already have your login data, please click here .
If you have forgotten your password you can you can recover it by clicking here and selecting the option ¿I have forgotten my password¿.



