

C0492 - CEREBRAL VASOSPASM FOLLOWING TRANSSPHENOIDAL PITUITARY ADENOMA SURGERY
1Servicio de Neurocirugía-Unidad de Raquis Quirúrgico; 2Servicio de Neurorradiología Intervencionista, Hospital Universitario Marqués de Valdecilla, Santander, Spain.
Objectives: Cerebral vasospasm is an extremely uncommon complication following transphenoidal surgery (TSS) of a pituitary adenoma. The etiology and physiopathology of this event is not well understood and several risk factors have been proposed. Given its low frequency the diagnosis and management is not clear either, that leads on an important morbidity and mortality. We present a case of vasospasm after TSS and we discuss about its etiology, diagnosis and management.
Methods: A 52 year-old woman presented with hirsutism of recent development. No neurologic deficits were found on physical examination. Endocrinological studies revealed elevated GH levels. A MRI was performed showing a pituitary macroadenoma of 3 × 3.4 × 2.8 cm with suprasellar extension and invasion of both cavernous sinuses. Surgical treatment was planned.
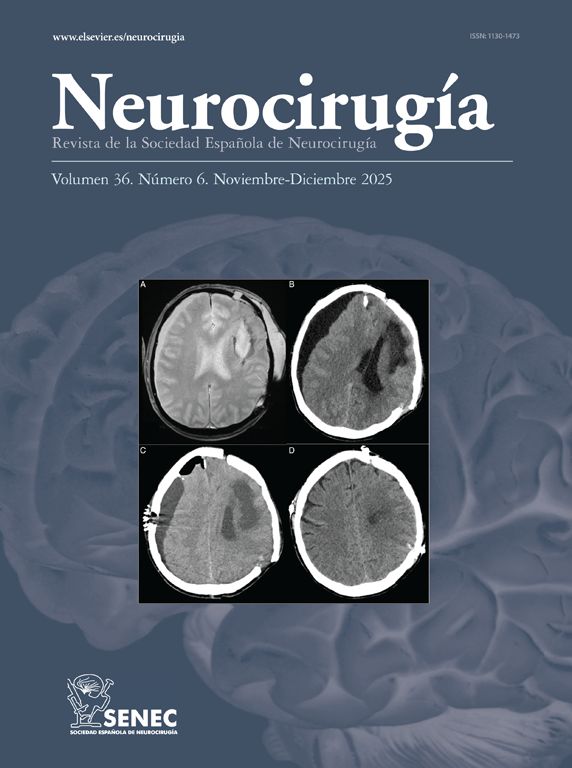
Results: The patient underwent an endoscopic expanded transsphenoidal transplanum approach. A lumbar drainage was placed for closure. Post-operative CT scan showed an extensive subarachnoid hemorrhage (SAH) filling the basal cisterns, without ventricular dilatation. Initially the post-operative period was uneventful, removing lumbar drainage on 6th day. However, the patient presented hard-to-handle hypertension, that was finally controlled on post-operative 6th day. On 7th day, she developed an abrupt neurological deficit, with mixed aphasia and right facial palsy. An urgent arteriography was performed, and it showed left middle cerebral artery vasospasm, so intra-arterial nimodipine was administered. After that, vasospasm disappeared and the patient recovered completely. She was discharged without neurological deficits after 16 days of hospitalization.
Conclusions: Cerebral vasospasm is a rare complication following TSS. The key to successful management is a high index of suspicion and early proactive management. The presence of postoperative SAH seems to definitely contribute to its apparition. Therefore, given the lack of evidence for the optimal management of these patients, treatment in concordance with protocols for vasospasm due to SAH is recommended.



